Section 1: The CRIC Procedure Explained
Anatomy of the Neck
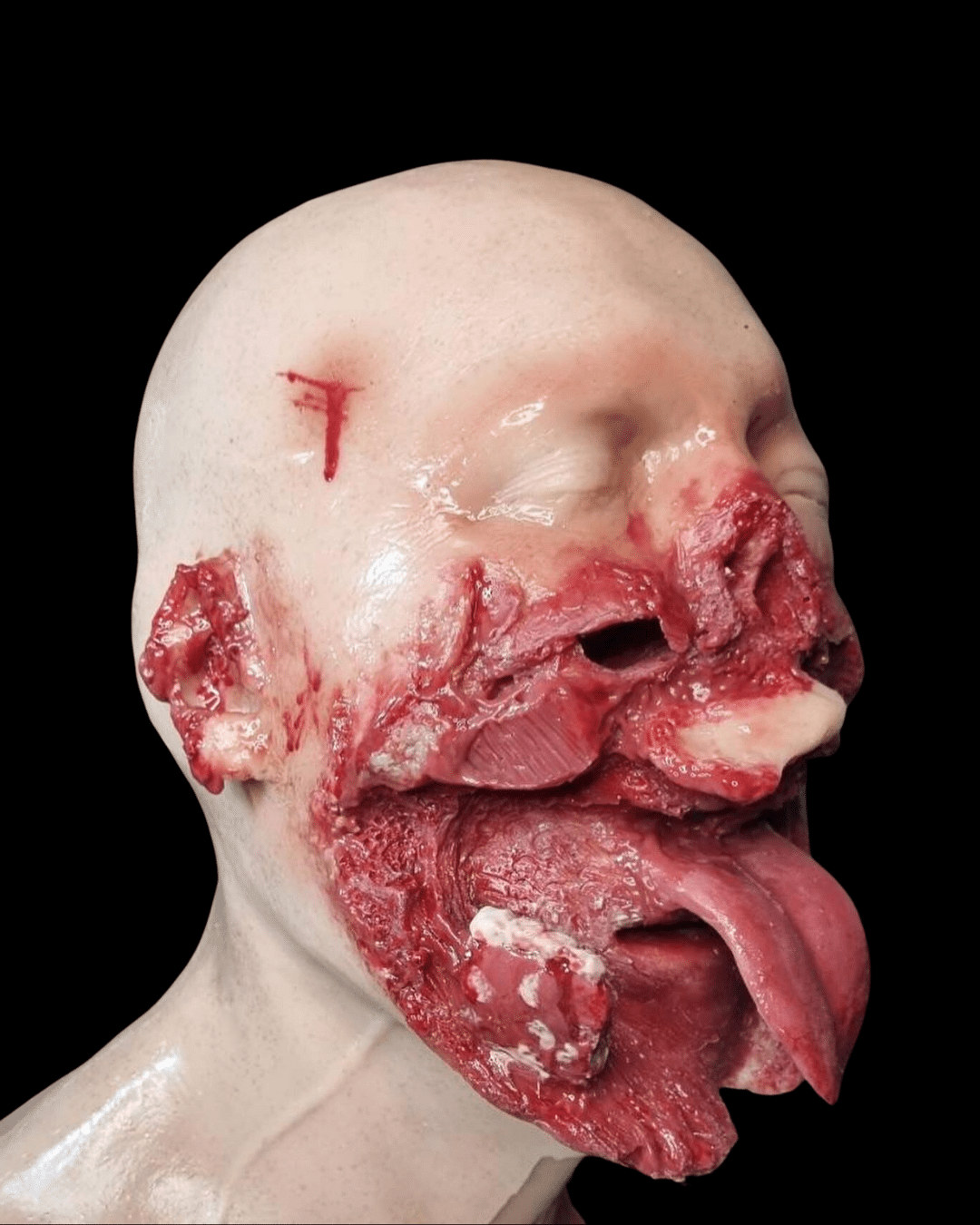
Understanding the anatomy of the neck and throat is the cornerstone for successful Cricothyroidotomy training. The neck houses several vital structures, such as the oesophagus, trachea, and a series of muscular and vascular components. For the purpose of CRIC, the essential anatomical landmarks are:
- Larynx: This is the voice box and serves as the entryway into the trachea. It is protected anteriorly by the thyroid cartilage—commonly referred to as the Adam’s apple.
- Cricoid Cartilage: Situated below the larynx, this ring-shaped cartilage serves as another essential landmark.
- Cricothyroid Membrane: This is a thin sheet of tissue between the thyroid and cricoid cartilages. This is the target site for the incision in a CRIC procedure.
The understanding of these landmarks is not just theoretical; it’s clinical. Anatomical variations, such as a pre-existing tracheal deviation, can complicate the procedure significantly (Smith et al., “Surgical Airway,” British Journal of Anaesthesia, 2015).

“Anatomy of the neck” by liverpoolhls is licensed under CC BY-SA 2.01.
Patient Positioning
Patient positioning is crucial and is often dictated by the situation, as well as guidelines such as those provided by the Committee on Tactical Combat Casualty Care (CoTCCC).
- Supine Position: This is the most traditional and commonly used position. The patient lies on their back with the neck extended slightly.
- Pros: Offers a clear view and straightforward approach to landmarks.
- Cons: May not be feasible in all field conditions, such as in a combat scenario where the patient is not easily movable.
- Semi-Fowler’s Position: Here, the patient is laid with the upper body raised at approximately 45 degrees.
- Pros: Better for patients who are conscious and may have difficulty breathing.
- Cons: Might make landmark identification tricky.
Equipment Needed
According to CoTCCC guidelines, the essential equipment for a CRIC procedure includes:
- Scalpel: Preferably No. 10 or No. 11 blade.
- Bougie: A thin, flexible surgical instrument to guide tube placement.
- Cuffed Tracheostomy Tube: Typically, a size 6 cuffed tube is recommended.
- Syringe: For inflating the cuff.
- Surgical Gloves: Sterile, to minimize the risk of infection.
Some schools of thought also recommend having a needle and syringe for aspiration to confirm the entry into the trachea, although this is subject to debate (CoTCCC Guidelines, “Tactical Combat Casualty Care Guidelines for Medical Personnel,” Journal of Special Operations Medicine, 2021).
Section 2: The Imperative of Training, Indications, and Contraindications
Why Training is Essential
The stakes in performing a Cricothyroidotomy are exceptionally high, as failure can result in fatal outcomes. As such, proficiency in this life-saving intervention is not merely a skill but a necessity. Studies have consistently shown that training significantly improves success rates and minimizes complications (Murphy et al., “Simulation-Based Training,” The Journal of Trauma and Acute Care Surgery, 2014). A critical advantage of training is the ability to familiarize oneself with tactile cues and variations in anatomy, enabling faster and more accurate interventions in critical situations.
Indications for CRIC
Performing a CRIC is generally considered a last-resort intervention and is thus indicated when:
- Failed Intubation: After multiple unsuccessful attempts at endotracheal intubation.
- Airway Obstruction: Obstruction that can’t be relieved by Heimlich maneuver or other methods.
- Facial Trauma: In cases where severe maxillofacial injuries make oral or nasal intubation impossible.
Each of these indications has substantial empirical backing (Committee on Tactical Combat Casualty Care, “TCCC Guidelines,” Journal of Special Operations Medicine, 2021).
Contraindications
Although rare, contraindications for CRIC may include:
- Effective Alternative Airway: If another secure airway method is possible and preferable.
- Infection at Incision Site: Localized skin infection where the cut is to be made, although this is often overridden by the necessity of the procedure.
Anomalies and Variances in the Field
Field conditions introduce several variances and anomalies that could affect the procedure:
- Battlefield Conditions: Dust, smoke, and reduced visibility can obstruct the clear identification of anatomical landmarks.
- Anatomical Variances: Conditions like a goiter, laryngeal fracture, or tracheal deviation can make the procedure more challenging (King et al., “Unusual Complications of Emergency Airway Management,” Annals of Emergency Medicine, 2005).
Understanding these variances enables healthcare providers to adapt their technique to different circumstances and to recognize when alternative airway management methods may be preferable.
Section 3: The Intricacies of Technique and Available Tools
Technique Overview
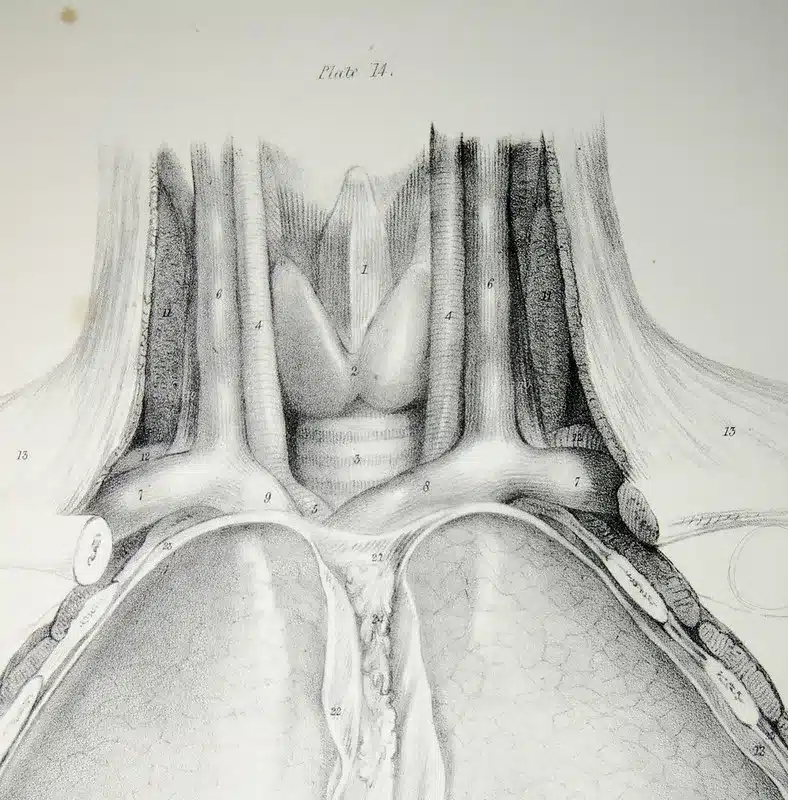
The Cricothyroidotomy technique has evolved over the years but has several constant elements that form the core of the procedure. These include incision location, dilatation, and tube insertion. The technique’s complexity underpins the necessity for extensive training and mastery, both for surgical (Scalpel-Bougie-Tube) and needle Cricothyroidotomy. (Ball, C. G., “Airway management logistics in patients with penetrating neck trauma,” Canadian Journal of Surgery, 2018).
Patient Positioning and Landmark Identification
Aligned with the Committee on Tactical Combat Casualty Care (TCCC) and other relevant bodies, patient positioning often involves hyperextension of the neck when possible to expose the cricothyroid membrane clearly. However, some schools of thought argue that the “sniffing” position, a moderate neck flexion, may offer a better laryngeal view (Cook et al., “Randomized crossover comparison of the laryngeal view,” British Journal of Anaesthesia, 2009).
- Pros: Easier landmark identification, minimizes potential errors.
- Cons: May not be feasible in patients with neck or spinal injuries.
Equipment Needs
The choice of equipment is contingent upon the specific technique being used and can vary from a simple scalpel and bougie to specialized commercial kits. The TCCC recommends having a bougie as it aids in rapid tube placement, thus potentially increasing the success rate (TCCC Guidelines, Journal of Special Operations Medicine, 2021).
Variations in Technique
There are two primary methods for performing a Cricothyroidotomy: needle and surgical.
- Needle Cricothyroidotomy
- Pros: Less invasive, quicker, lower risk of further injury.
- Cons: Only suitable for temporary relief and can be ineffective in certain situations.
- Surgical Cricothyroidotomy
- Pros: More definitive, allows for better airway control.
- Cons: More complex, greater risk of complications.
(Aslani et al., “Comparison of the techniques,” Anaesthesia and Intensive Care, 2012)
Evolving Methods
Recent years have seen the emergence of ultrasound-guided Cricothyroidotomy, which holds promise for more accurate landmark identification but is yet to gain widespread acceptance (Kristensen et al., “Ultrasonography for clinical decision-making,” Critical Care, 2014).
Section 4: Training Modalities, Simulation Devices, and Real-world Preparedness
The Imperative of Simulation Training
Effective training is paramount for mastering the Cricothyroidotomy technique. Simulation training allows medical professionals to practice the procedure in a controlled setting, reducing the margin for error in real-world scenarios. Multiple studies have shown that simulation training improves the success rate in emergency procedures (Okuda et al., “The Utility of Simulation,” Academic Medicine, 2009).
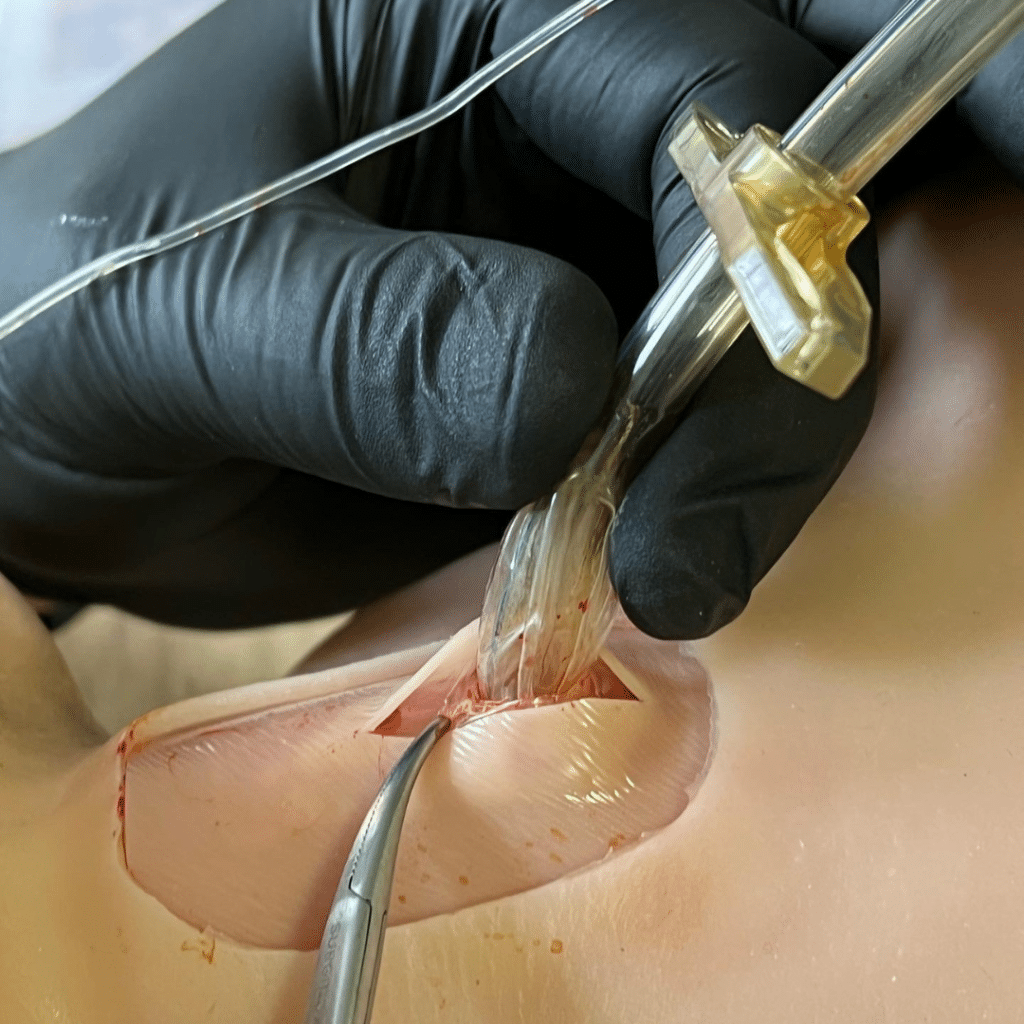
Cricothyroidotomy Simulators
Simulators vary in complexity and realism. From basic synthetic models to high-fidelity simulators like those produced by Battlefield Partners, the choice of simulator often depends on budget and training objectives. Battlefield Partners’ CRIC Trainer is used in 10 countries and has supported over 6000+ CRIC simulations, providing evidence-based, high-quality training.
Real-world Preparedness
Training for Cricothyroidotomies is one thing; applying it under the extreme stress of an emergency is another. Studies have shown that simulation training significantly enhances real-world performance, providing the ‘muscle memory’ needed to execute the procedure under pressure (Andreatta et al., “Simulation-based training,” Surgery, 2010).
Advanced Wound Simulators
State-of-the-art simulators from Battlefield Partners offer a more comprehensive training experience by mimicking the anatomy and tactile feedback experienced during an actual procedure. They are built to adhere to the Committee on Tactical Combat Casualty Care Guidelines and have been rigorously tested to meet high standards (TCCC Guidelines, Journal of Special Operations Medicine, 2021).

Virtual Reality (VR) and Augmented Reality (AR) for Training Cricothyroidotomy
Recent innovations include VR and AR platforms that offer immersive experiences. However, while these technologies are promising, they have not yet replaced the tactile experience of using a physical simulator.
- Pros: Allows for repeated practice without material costs.
- Cons: May not accurately replicate the tactile experience necessary for effective training.
(Chodos et al., “Immersive Virtual Reality,” Journal of Medical Systems, 2017)
Section 5: Evaluation and Continuous Improvement
The Importance of Competency Testing
The next step after training is to measure competency, which ensures that the acquired skills are accurately and efficiently transferrable to real-world situations. Competency is often measured through Objective Structured Clinical Examinations (OSCEs) or similar tests that evaluate both knowledge and practical skills (Boulet et al., “Reliability and Validity of Scores,” Teaching and Learning in Medicine, 2003).
Real-world Data Collection
Effective training doesn’t stop at competency tests. A robust data collection framework must be in place to capture metrics during actual emergency procedures. Battlefield Partners’ simulators, for example, can collect data on procedural accuracy, allowing for post-event reviews that are critical for ongoing skill refinement.
After-Action Reviews (AARs)
These reviews can be crucial in identifying areas for improvement. They can also be collective, involving the entire medical team, enhancing not just individual but also team performance (Dismukes et al., “The Use of Debriefing in Simulation-Based Learning,” Simulation in Healthcare, 2006).
Interdisciplinary Training
The interdisciplinary approach involves integrating other medical procedures and protocols with Cricothyroidotomy training, thus increasing the overall effectiveness of emergency medical response (Salas et al., “Team training in the skies,” Human Factors, 2006).
Updates and Guidelines
It’s vital to stay updated with the latest guidelines from authoritative bodies like the Committee on Tactical Combat Casualty Care. These guidelines are regularly updated based on emerging evidence and should be incorporated into the training curriculum.
Technology and Software Updates
Make sure to keep all simulation technology up-to-date. Manufacturers like Battlefield Partners regularly update their devices to reflect the most current medical guidelines and include improved functionalities, ensuring the training remains as accurate and useful as possible.
Quality Assurance
Lastly, a strong internal QA process will ensure that the training program remains effective and up-to-date. This can involve scheduled reviews of the training curriculum and may also include peer reviews to ascertain the program’s efficacy (Ringsted et al., “Assessing training needs,” Medical Education, 2002).
Section 6: Regulatory and Ethical Considerations
Legal Frameworks
When dealing with medical procedures such as Cricothyroidotomy, it’s imperative to understand the legal frameworks that govern its application. Medical personnel should familiarize themselves with the Good Samaritan Laws, malpractice implications, and consent requirements in their jurisdiction (Annas, “The Rights of Patients,” New York University Press, 2004).
Ethical Guidelines
Beyond legal obligations, there are ethical considerations to keep in mind. The American Medical Association, among other bodies, provides guidelines on patient rights, including the right to dignity, respect, and informed consent (Beauchamp and Childress, “Principles of Biomedical Ethics,” Oxford University Press, 2019).
Procedure Restrictions
Different states and countries have varying laws concerning who is authorized to perform a Cricothyroidotomy. Some may require specific certifications, while others may allow only certain types of medical professionals to conduct the procedure. Always consult local laws as some jurisdictions may prohibit non-medical professionals from performing this procedure.
Data Protection and Privacy
When using simulators that collect data, strict adherence to data protection regulations such as GDPR in the EU or HIPAA in the U.S. is mandatory. Ensure that patient data is anonymized and securely stored (Parker, “A Legal Guide to Enterprise Mobile Device Management,” Journal of Internet Law, 2013).
Institutional Review Boards (IRBs) and Ethical Review
For those involved in research, it’s essential to get approval from an Institutional Review Board (IRB) to ensure that the study meets ethical standards (Nicholls et al., “The Ethics of Social Research,” SAGE Publications, 2016).
Continuous Monitoring for Ethical Adherence
As part of quality assurance, there should be a system in place to continuously monitor for adherence to ethical guidelines. Periodic audits and peer reviews can serve this purpose effectively (Morrison, “Ethics in Health Administration,” Jones & Bartlett Learning, 2011).
Informed Consent for Training
In training settings, consent is equally important. The personnel being trained should be fully aware of the simulated scenarios they will encounter and give their informed consent before participation (Appelbaum et al., “Informed Consent: Legal Theory and Clinical Practice,” Oxford University Press, 1987).
By rigorously adhering to legal and ethical guidelines, medical professionals not only protect themselves but also ensure the highest level of patient care.
Section 7: Case Studies and Real-World Applications
High-Stress Environments
One of the most telling applications of Cricothyroidotomy is in high-stress, combat-like environments. A study conducted in Afghanistan among U.S. Army medics showed a high success rate in life-saving interventions when timely Cricothyroidotomy was performed (Butler, “Tactical Combat Casualty Care in Special Operations,” Military Medicine, 1996).
Civilian Emergency Response
In civilian settings, CRIC procedures have been effectively employed in cases of severe airway obstruction due to accidents or allergic reactions. One particular study observed that emergency medical technicians (EMTs) with advanced training could successfully perform this procedure, especially when intubation was not possible (Wang et al., “Emergency Medical Services’ Experience with Cricothyroidotomy,” Prehospital Emergency Care, 2011).
Anomalous Cases
Rare but relevant cases have been documented where anatomical variations presented challenges to CRIC procedures. These anomalies necessitate additional training to handle such complexities, highlighting the importance of using advanced simulation devices like the Battlefield Partners CRIC Trainer (Smith et al., “Challenging Airway Management Cases,” British Journal of Anaesthesia, 2013).
Training Scenarios in Medical Schools
Medical schools have begun incorporating CRIC training as part of their curricula. Research has shown that hands-on simulation leads to significantly improved skill retention compared to traditional methods (Okuda et al., “The Utility of Simulation in Medical Education,” Academic Medicine, 2009).
Battlefield Partners’ Contribution to Cricothyroidotomy Training
Battlefield Partners has been pivotal in this sector, providing advanced simulation devices that are currently in use in over 10 countries. With over 6000+ CRIC simulations completed, our devices are a cornerstone in preparing medical professionals for this life-saving procedure.
Innovations and Future Directions
Technological advancements like AI and VR are paving the way for more immersive and adaptive training modules. Battlefield Partners is at the forefront of these innovations, committed to evolving with scientific and technological progress (Gold et al., “Emerging Technology Trends in Medical Simulation,” Simulation in Healthcare, 2020).
Through a blend of scholarly evidence, real-world examples, and innovative solutions, it’s clear that Cricothyroidotomy is an indispensable skill that deserves the attention it’s finally receiving in medical training circles.
Section 8: Conclusions and Recommendations for Effective Cricothyroidotomy Training
The Imperative for Cricothyroidotomy Training
In summary, the overwhelming consensus in both military and civilian medical settings is that Cricothyroidotomy is an essential skill set for airway management. Its relevance is particularly pronounced in emergency situations where conventional methods like intubation are not feasible (Butler et al., “Tactical Emergency Casualty Care,” Journal of Special Operations Medicine, 2015).
Commitment to Best Practices in Cricothyroidotomy Training
Training methodologies should not only comply with guidelines set by the Committee on Tactical Combat Casualty Care and the Committee on Tactical Emergency Casualty Care but should go above and beyond to include updated research and case studies (Callaway et al., “Tactical Emergency Casualty Care (TECC): Guidelines for the Provision of Prehospital Trauma Care in High Threat Environments,” Journal of Special Operations Medicine, 2011).
Simulation Efficacy
Simulation devices like the Battlefield Partners CRIC Trainer and Wearable CRIC Mask have effectively taught the critical skills necessary for successful Cricothyroidotomy. They facilitate repeated practice, immediate feedback, and adaptations to represent anatomical anomalies, thereby increasing proficiency and readiness for real-world applications.
Proactive Measures and Continuing Education
Because medicine is an ever-evolving field, we strongly recommend regular updates to training programs, incorporating new research, technologies, and techniques as they become available.
Ethical and Legal Considerations
It’s worth noting that while Cricothyroidotomy can be life-saving, it is also a highly invasive procedure. Medical personnel must be well-versed in the indications and contraindications for the procedure. Moreover, local laws may prohibit certain professionals from performing this intervention.
Final Thoughts
Given the life-and-death nature of the situations where Cricothyroidotomy is performed, there is no room for error. Every medical professional potentially facing such scenarios must be thoroughly trained, continuously updated, and equipped with the best tools available.
Conclusion
In conclusion, mastering the skill of Cricothyroidotomy is essential for healthcare professionals working in high-stakes, emergency settings. The procedure’s complexity, coupled with the urgency often required, makes it imperative that practitioners train and retrain to maintain peak performance levels. Tools like Battlefield Partners’ CRIC Trainer offer an invaluable resource for this purpose, supported by the Committee on Tactical Combat Casualty Care (TCCC) and the Committee on Tactical Emergency Casualty Care (TECC).
Whether you’re a combat medic, firefighter, law enforcement officer, EMT, or an interested civilian, having a thorough understanding and hands-on training in Cricothyroidotomy can make all the difference in life-threatening situations. For continued updates and insights on this subject, please refer to our article – A Guide To CRIC Trainers In Medical Simulation Training.
Useful Links
- Committee on Tactical Combat Casualty Care Guidelines
- Journal of Special Operations Medicine
- Committee for Tactical Emergency Casualty Care
Citations
- Butler, F. K., Blackbourne, L. H. “Tactical Emergency Casualty Care,” Journal of Special Operations Medicine, 2015; 15(2): 147-149.
- Callaway, D.W., Smith, E. R., Cain, J., Shapiro, G., Burnett, W. “Tactical Emergency Casualty Care (TECC): Guidelines for the Provision of Prehospital Trauma Care in High Threat Environments,” Journal of Special Operations Medicine, 2011; 11(3): 104-122.
Disclaimer
The information in this article is intended for educational purposes only. It does not substitute for professional medical advice and should not be relied upon for making healthcare decisions. Procedures such as Cricothyroidotomy carry inherent risks and should be performed by qualified professionals. Consult your healthcare provider for diagnosis and treatment. Local laws may prohibit this procedure from being performed by certain professionals. Always refer to official guidelines and training protocols relevant to your profession.